Imagine a non-invasive therapy that uses magnetic pulses to stimulate the brain, offering hope for individuals struggling with depression, anxiety, and even neurological disorders. This is the promise of Transcranial Magnetic Stimulation (TMS)—a groundbreaking technique that has revolutionized mental health treatment.
Originally developed in the 1980s, TMS has gained widespread recognition for its ability to modulate brain activity without the need for surgery or medication. Whether used to alleviate treatment-resistant depression or explore cognitive enhancement, TMS represents a significant step forward in neuroscience and psychiatry.
In this blog, we’ll explore how TMS works, its benefits, potential side effects, and the latest advancements in this fascinating field. Could TMS be the future of brain therapy? Let’s dive in.
Transcranial Magnetic Stimulation
Over the past few decades, advancements in neuroscience have significantly improved non-invasive brain stimulation techniques 2, particularly in conscious individuals. Among these innovations, Transcranial Magnetic Stimulation (TMS) has emerged as a promising treatment option for mental health conditions, especially when traditional approaches such as medication and counselling prove ineffective.
Key Advantages of TMS:
- Non-invasive and well-tolerated: TMS does not require anaesthesia and is generally considered safe with minimal discomfort.
- Convenient outpatient procedure: Patients can undergo treatment without disrupting their daily routines.
- Proven efficacy: Research supports its effectiveness, particularly in individuals who have not responded to conventional treatments.
- Alternative for treatment-resistant patients: TMS offers hope for those who struggle with medication-resistant depression and other psychiatric conditions.
Brief History of TMS
The concept of using electromagnetic fields to influence brain activity dates back to the 19th century when Michael Faraday discovered the principles of electromagnetic induction. However, the practical application of Transcranial Magnetic Stimulation (TMS) did not emerge until 1985, when Anthony Barker and his colleagues developed the first TMS device at the University of Sheffield, UK (Barker et al., 1985). Since then, TMS has evolved significantly, gaining regulatory approvals for clinical applications in depression, obsessive-compulsive disorder (OCD), and other neurological conditions.
Brain stimulation therapies play a crucial role in treating mental disorders and other psychiatric conditions. These therapies work by modulating brain activity through the application of external magnetic fields, a process known as electromagnetic induction, where electrical energy is converted into magnetic energy.
Since 1985, TMS is widely used for various mental health and neurological conditions. The foundation for TMS was laid in 1980 when Merton and Morton successfully stimulated the motor cortex using transcranial electrical stimulation (TES). However, due to the discomfort associated with TES, Anthony T. Barker sought an alternative approach. His research into the use of magnetic fields to influence electrical signalling in the brain led to the development of the first stable TMS devices in 1985.4
Finally, TMS devices got the approval of United States’ FDA (Food & Drug Administration – USA) first in October 2008.
How TMS Works
TMS is a non-invasive brain stimulation technique that uses electromagnetic fields to stimulate specific areas of the brain.1 It primarily targets the prefrontal cortex, which plays a crucial role in mood regulation. Unlike traditional treatments such as medication or electroconvulsive therapy (ECT), TMS does not require anaesthesia, making it a well-tolerated option for many individuals.
TMS is a procedure that uses magnetic fields to modulate brain activity, influencing the communication between neurons. Since neurons naturally use tiny electrical impulses to send and receive signals throughout the brain and body, TMS harnesses this principle to stimulate specific brain regions non-invasively.5
The technology behind TMS is based on electromagnetic induction, a principle discovered by Michael Faraday in the 19th century. A TMS device consists of a coil that generates magnetic fields, which penetrate the skull and induce electrical activity in the targeted brain regions. These magnetic pulses influence neural circuits involved in mood regulation, gradually restoring the normal activity of brain cells that may be underactive in conditions such as depression.
Role of Coils in Transcranial Magnetic Stimulation (TMS) Treatment
Coils play a fundamental role in Transcranial Magnetic Stimulation (TMS) by generating the magnetic fields necessary to induce electrical activity in targeted brain regions. The effectiveness, depth of stimulation, and focality of TMS treatment largely depend on the design, shape, and positioning of the coil used.
Mechanism of Action
TMS coils create rapidly changing magnetic fields that penetrate the scalp and skull to induce an electric current in underlying cortical neurons. This induces or modulates neural activity without the need for direct electrical contact.
Typically, TMS is considered when standard treatments, such as psychotherapy and pharmacological interventions, fail to alleviate symptoms of mental illnesses like major depressive disorder (MDD), obsessive-compulsive disorder (OCD), and other neuropsychiatric conditions.
Three Basic Types of TMS are available:
- Single-Pulse: Single-pulse transcranial magnetic stimulation (TMS) is a non-invasive technique that applies a brief magnetic pulse to a specific brain region. This pulse generates electrical currents in the underlying neural tissue, temporarily stimulating or modulating brain activity. Single-pulse TMS is widely used to examine the timing of fundamental brain processes and assess cortical circuit excitability. Single-pulse transcranial magnetic stimulation (sTMS) is an innovative therapy for acute migraine relief.30
- Paired-Pulse TMS: Primarily used for research purposes to study brain function and connectivity. Paired pulse transcranial magnetic stimulation allows for the exploration of both intra-cortical connections within a specific brain region and inter-cortical connections between different brain regions.
In paired-pulse stimulation, two pulses are delivered out of phase to either modulate neuronal activity within the same hemisphere by inducing inhibition or excitation or to simultaneously inhibit neurons in one hemisphere while exciting those in the opposite hemisphere.31
- Repetitive TMS (rTMS): Repetitive transcranial magnetic stimulation (rTMS) is the most extensively utilized TMS technique throughout the history of transcranial magnetic stimulation. Used in clinical settings to induce prolonged changes in brain activity, potentially leading to long-term symptom relief.
Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive therapy that utilizes magnetic fields to deliver repeated low-intensity pulses, stimulating targeted areas of the brain. The strength of the magnetic field generated by rTMS is comparable to that of a Magnetic Resonance Imaging (MRI) scan2. The magnetic field works like Magnetic Resonance Imaging (MRI) 3, and typically, these pulses penetrate only a few centimetres into the brain unless specialized coils and techniques are used to achieve deeper stimulation. 4
Factors affecting the efficiency of TMS, including:
- Frequency and duration of stimulation
- Magnetic pulse intensity
- Coil shape and orientation
- Excitability of the targeted neural circuits
By generating a magnetic field through a wire coil placed on the scalp, TMS can modulate brain excitability and neural plasticity. Research indicates that repetitive TMS (rTMS) can induce lasting changes in brain function, making it a valuable tool for both neurological research and therapeutic interventions.
Over the past decades, advancements in non-invasive brain stimulation techniques have significantly benefited neuroscience research. One such method, Transcranial Magnetic Stimulation (TMS), delivers electrical stimuli through the scalp in conscious individuals. Generally, single-pulse TMS (including paired-pulse TMS) is employed to investigate brain function, while repetitive TMS (rTMS) is used to induce lasting changes in brain activity beyond the stimulation period.
As Transcranial Magnetic Stimulation (TMS) gained popularity for its effectiveness, ongoing research has led to greater specialization, resulting in the development of additional brain-related treatments that benefit humanity.
Other types of TMS:
- Theat Burst Stimulation (TBS)
- NAVIGATED TMS (nTMS)
- Quadri-pulse Stimulation
- Deep TMS
In single-pulse TMS, a single magnetic pulse is delivered at intervals of several seconds or longer. In contrast, repetitive transcranial magnetic stimulation (rTMS) has become increasingly popular for its ability to deliver magnetic stimulation at a consistent, rhythmic frequency over an extended period.
In repetitive transcranial magnetic stimulation (rTMS), magnetic pulses are delivered in rapid sequences, known as “trains.” This technique involves the administration of multiple single-pulse stimuli at a predetermined frequency, intensity, and duration, leading to either excitation or inhibition of activity in the targeted cortical region.
For instance, slow rTMS at a frequency of 1 Hz, which has an inhibitory effect, delivers one magnetic pulse per second. In contrast, fast rTMS at 10 Hz, which is excitatory, administers ten magnetic pulses per second.6
While repetitive transcranial magnetic stimulation (rTMS) has demonstrated effectiveness in treating depression, individual responses to the treatment vary significantly. A more recent rTMS protocol, known as theta-burst stimulation (TBS), has been found to elicit comparable or even greater effects on brain activity than standard rTMS. One key advantage of TBS is its significantly shorter administration time. Traditional rTMS sessions typically range from 20 to 45 minutes, whereas TBS protocols require only 1 to 3 minutes of stimulation.7
Repetitive transcranial magnetic stimulation (rTMS) was originally introduced as a treatment for major depressive disorder (MDD) in patients who did not respond to conventional antidepressant therapies. As rTMS technology advances, newer protocols such as Theta-Burst Stimulation (TBS) have emerged, offering distinct advantages over traditional rTMS approaches.
Theta-burst stimulation (TBS) is a more recent advancement in repetitive transcranial magnetic stimulation (rTMS). The shorter duration of TBS treatments allows for increased treatment capacity and potentially lower costs per session. 29
Multiple TBS clinical protocols have demonstrated efficacy in treating MDD, including intermittent TBS (iTBS) targeting the left dorsolateral prefrontal cortex (DLPFC)32, continuous TBS (cTBS) applied to the right DLPFC, and a sequential bilateral approach combining cTBS on the right DLPFC followed by iTBS on the left DLPFC within the same session.8
Theta Burst Stimulation (TBS) is a refined form of repetitive Transcranial Magnetic Stimulation (rTMS) that mimics the natural theta rhythms observed in the human brain. This technique delivers bursts of high-frequency magnetic pulses in a patterned sequence, modulating cortical excitability and inducing neuroplastic changes. Due to its ability to alter synaptic activity efficiently, TBS has gained significant attention in neuromodulation research and clinical applications.
Types of Theta Burst Stimulation (TBS)
There are two main protocols for delivering TBS:
- Intermittent Theta Burst Stimulation (iTBS):
- In iTBS, bursts of stimulation are delivered intermittently, allowing for periods of rest between stimulations.
- This protocol has been shown to increase cortical excitability, making it a potential tool for cognitive and motor function enhancement.
- Studies have demonstrated that applying iTBS to the primary motor cortex leads to an increase in the amplitude of motor-evoked potentials (MEPs), suggesting a facilitatory effect on neural activity.
- iTBS has been investigated for its potential in treating major depressive disorder (MDD), cognitive dysfunction, and post-stroke rehabilitation.
- Continuous Theta Burst Stimulation (cTBS):
- In contrast, cTBS delivers bursts continuously without intervals, leading to a sustained inhibitory effect on cortical excitability.
- Research indicates that cTBS applied to the motor cortex 47 results in reduced motor activity, suggesting its potential for conditions associated with excessive cortical excitability 48, such as epilepsy or movement disorders.
- The suppressive effects of cTBS are thought to be mediated through long-term depression (LTD)-like synaptic mechanisms, making it a valuable tool in experimental neuroscience.
Mechanisms of Action: Neuroplasticity 49 and Synaptic Modulation 50
Theta Burst Stimulation exerts its effects through synaptic plasticity, which is the brain’s ability to strengthen or weaken synaptic connections in response to activity. The two main processes involved in TBS are:
- Long-Term Potentiation (LTP): Associated with iTBS, this mechanism strengthens synaptic connections, enhancing neuronal communication and cognitive functions.
- Long-Term Depression (LTD): Linked to cTBS, this process weakens synaptic activity, leading to a reduction in cortical excitability.
These mechanisms parallel natural processes involved in learning and memory formation, which is why TBS has been extensively studied in the context of cognitive enhancement and psychiatric disorders.
Clinical Applications of Theta Burst Stimulation
TBS has shown promise in various neurological and psychiatric disorders, including:
- Major Depressive Disorder (MDD):
- iTBS targeting the left dorsolateral prefrontal cortex (DLPFC) has demonstrated antidepressant effects similar to conventional rTMS but with shorter treatment durations.
- Studies suggest that iTBS sessions can be completed in just 3 minutes, compared to the traditional 37-minute rTMS protocols.
- The U.S. FDA has approved iTBS for the treatment of treatment-resistant depression, making it a practical and efficient alternative to traditional rTMS.
- Post-Traumatic Stress Disorder (PTSD):
- Emerging research suggests that iTBS applied to the DLPFC can help modulate emotional processing and reduce hyperarousal symptoms in PTSD patients.
- A study published in Frontiers in Psychiatry found that accelerated iTBS protocols could lead to significant symptom reductions in PTSD.
- This opens new avenues for non-invasive neuromodulation in trauma-related disorders.
- Cognitive Enhancement and Neurorehabilitation:
- iTBS has been investigated for memory improvement, attention enhancement, and learning facilitation in both healthy individuals and patients with Alzheimer’s disease.
- In stroke rehabilitation, TBS has shown potential in improving motor recovery, particularly when applied to the motor cortex of the affected hemisphere.
- Research suggests that a combination of iTBS on the affected side and cTBS on the unaffected hemisphere can improve motor function by restoring balance between the two hemispheres.
- Parkinson’s Disease and Movement Disorders:
- TBS has been explored as a treatment for Parkinson’s disease, where it may help modulate abnormal cortical activity and improve motor symptoms.
- Some studies suggest that iTBS could enhance dopaminergic function, offering a potential non-pharmacological approach to symptom management.
- Pain Management and Fibromyalgia:
- Chronic pain conditions, including fibromyalgia, have been linked to dysregulated cortical excitability.
- iTBS over the primary motor cortex (M1) has been found to reduce pain perception and improve quality of life in chronic pain patients.
- The analgesic effects of TBS are thought to be mediated through central pain modulation mechanisms. 41
Advantages of Theta Burst Stimulation Over Traditional rTMS
- Time Efficiency: iTBS sessions last only a few minutes compared to conventional rTMS, making it more accessible and patient-friendly.
- Equivalent or Superior Efficacy: Studies suggest that iTBS can achieve the same or even better therapeutic effects than traditional rTMS, especially in depression treatment.
- Lower Stimulation Intensities: TBS protocols often use lower intensities while maintaining their therapeutic effects, potentially reducing side effects. 40
Limitations and Challenges
Despite its advantages, TBS also has limitations:
- Variability in Response: Not all patients respond equally to TBS, and individual factors such as brain anatomy, baseline cortical excitability, and genetics may influence outcomes.
- Standardization Issues: Different studies use varying stimulation parameters, leading to inconsistencies in results.
- Potential Side Effects: While generally well-tolerated, TBS may cause mild headaches, scalp discomfort, or rare seizures in susceptible individuals. 39
Future Directions and Research Trends
The field of TBS continues to evolve, with ongoing research exploring:
- Personalized Stimulation Protocols: Using AI and neuroimaging to tailor TBS parameters for individualized treatments.
- Combination Therapies: Investigating TBS alongside pharmacotherapy, cognitive training, or brain-computer interfaces to enhance outcomes.
- New Target Regions: Expanding applications to treat cognitive impairments, addiction, and neurodevelopmental disorders.52
Safety and Efficacy of Theta Burst Stimulation (TBS)
Clinical studies on TBS indicate that TBS was not found to have higher rates of side effects or poorer safety profiles in comparison to standard rTMS. In both the conventional form of rTMS as well as TBS the common side effects includes headaches and fatigue. There is a very minimal risk of seizures in both forms of Transcranial magnetic stimulation (TMS). TBS when applied to the frontal cortices is associated with antidepressant effects which are of equal if not greater than the convention rTMS high frequency treatments.26
Although TMS is generally regarded as safe, risks are increased for therapeutic rTMS compared to single or paired diagnostic TMS. 27
Adverse effects of TMS are rare and may include fainting or seizures. Other potential concerns involve discomfort, pain, and unintended current induction in implanted medical devices such as pacemakers or defibrillators.39
Adverse effects generally increase with higher frequency stimulation (amplitude).28
However, Global community is having a consensus conference, promoted and supported by the International Federation of Clinical Neurophysiology (IFCN), which took place in Siena (Italy) in October 2018. The meeting aimed to revise and update the decade-old safety guidelines for the use of transcranial magnetic stimulation (TMS) in both research and clinical applications. (Rossi et al., 2009).
The 2009 recommendations established benchmarks for describing conventional and patterned TMS protocols, screening subjects and patients, implementing neurophysiological monitoring for new protocols, using reference stimulation thresholds, managing seizures, and documenting minor side effects.
From the meeting up to April 2020, additional safety concerns were extensively discussed, particularly regarding newly developed stimulation devices and pulse configurations, the responsibilities of device manufacturers, and emerging applications of TMS. These include its use in neuroimaging, imaging-guided and robot-assisted TMS, TMS combined with transcranial electrical stimulation, safety considerations in paired associative stimulation interventions, and the potential risks associated with using TMS for therapeutic seizure induction (magnetic seizure therapy).28
TMS is a promising technique in behavioural and physiology related brain issues.
TMS does not require surgery or electrode implantation. Its use can be divided into diagnostic and therapeutic applications. The effects of TMS depend on the frequency and intensity of the magnetic pulses, as well as the duration of treatment, which determines the total number of pulses delivered.
TMS treatments are approved by the FDA in the US and by NICE (National Institute for Health and Care Excellence – Government of UK), CE by European Union for the treatment of depression and are predominantly provided by private clinics.
Apart from therapies and procedures as mentioned above, some of the manufacturers claimed to have used TMS in healthcare application as peripheral magnetic stimulation to treat:
- pain
- spasticity and movement disorders
- facial and trigeminal neuropathy
- cough assist in bed bound patients
- after exercise muscle recovery
- physical exercise
- urology, proctology and gynaecology
- chronic pelvic pain syndrome
These treatments procedure is yet to get the FDA certificate. But one thing is certain that TMS procedure will go a long way to treat psychological, neurological and in some health issues in a most non-invasive way in near future
Theta Burst Stimulation represents a powerful advancement in the field of non-invasive brain stimulation, offering time-efficient and effective neuromodulation for both research and clinical applications. Its ability to induce neuroplasticity, regulate cortical excitability, and improve symptoms in neurological and psychiatric disorders makes it a promising tool for the future of neurotherapeutics. However, further research is needed to optimize protocols, improve response rates, and fully understand its long-term effects.
nTMS (Navigated Transcranial Magnetic Stimulation)
Navigated Transcranial Magnetic Stimulation (nTMS) is a non-invasive technique designed to stimulate specific cortical regions with precision. By enabling real-time visualization of the induced electric field, nTMS allows operators to accurately target anatomical loci within the cortex. Functioning as a stereotactic navigational system, nTMS relies on imaging techniques such as MRI to ensure the precise delivery of TMS pulses for targeted brain stimulation. 9
In this process, during the time of procedure, a coil transmits electrical currents that generate an electromagnetic field, which is directed through the head via an externally positioned device. This field seamlessly penetrates the scalp, skull, and cerebrospinal fluid, enabling precise external stimulation. When integrated with a frameless stereotactic navigational system, magnetic pulses can be accurately delivered to targeted brain regions, enhancing the effectiveness of navigated transcranial magnetic stimulation (nTMS) for both clinical and research applications. 42
Navigated transcranial magnetic stimulation (nTMS) is a well-established, non-invasive brain stimulation technique commonly used for preoperative mapping in neurosurgical patients. Beyond its surgical applications, nTMS holds promise for diagnosing and managing acute neurological injuries in inpatient settings with a shorter stay.
As an image-guided method, nTMS provides high precision, facilitating detailed assessments of neuromuscular pathway integrity, particularly in conditions such as spinal cord injury. Unlike transcranial electrical motor-evoked potentials, nTMS is both non-invasive and painless, making it suitable for bedside application without anaesthesia. Moreover, it does not require active patient participation, allowing its use in sedated patients, those unable to undergo comprehensive neurological examinations, and individuals in intensive care units (ICUs). 43
Given these advantages, successful integration of nTMS into neurocritical care could provide a valuable tool for objective and quantifiable neurological assessments in patients with suspected or confirmed neurological impairment. 10
Navigated TMS for better depression treatment
Hence, we can conclude that, nTMS is used to activate brain circuits in depressed brains. The question is, an nTMS be utilized similarly to pre-surgical mapping by neurosurgeons, offering improved accuracy in the treatment of MDD with TMS?. The results are encouraging.
Advantages of Navigated TMS Therapy
Navigated TMS treatments have been designed to be customized as per brain’s anatomy and alertness level which differs from person to person, and with following advantages:
- Better accuracy while defining the individualized dose of TMS
- Customised treatment sessions for individual brain.
- Enhanced safety and comfort with much less side effects
Three Variants of Navigated TMS Therapy for Depression
- Non-MRI Navigated TMS Therapy
Non-MRI Navigated TMS therapy determines the treatment target using the 5.5 cm rule rather than MRI-based software calculations. While this approach is less precise than the other two methods, it offers greater convenience by eliminating the need for an MRI and is also more cost-effective
- Structural-MRI Navigated TMS Therapy
This method requires a structural MRI and a radiologist’s assessment to identify the anatomical target, F3. The system then guides the operator to precisely target this location. While it provides greater structural accuracy than non-MRI navigation, it is less precise than functional connectivity MRI-navigated TMS. Additionally, MRI costs are typically not covered by insurance, and brain imaging is not necessary for diagnosing depression
In the treatment of depression (and some types of pain), the desired placement of the TMS coil is often above the left dorsolateral prefrontal cortex (DLPFC) which corresponds to the F3 location given by the 10–20 system.
The International 10–20 system is a method for standardized placement of electroencephalogram (EEG) electrodes. But 10-20 system requires special training and experience to use 10 – 20 system in TMS.
The F3 system requires less time and training to find the optimal position for prefrontal coil placement and it saves considerable time compared to the 10–20 EEG system. This system requires less time and training to find the optimal position for prefrontal coil placement and it saves considerable time compared to the 10–20 EEG system.11
Comparing the Reliability of Targeting Methods in TMS for Depression: Beam F3 vs. 5.5 cm Rule
Highlights
- Beam F3 and the 5.5 cm rule are two TMS targeting strategies for treating depression.
- Beam F3 offers greater precision in targeting compared to the 5.5 cm rule.
- This accuracy remains consistent across different time points, technicians, and test subjects
- These methods identify different prefrontal targets.11
Functional-MRI Navigated TMS Therapy
This approach has the greatest potential to transform the practice of TMS. The brain’s structural anatomy does not always align with its functional anatomy, making anatomical landmarks less reliable for precise targeting. Instead, functional MRI is used to individualize treatment, identifying the exact location of each patient’s functional dorsolateral prefrontal cortex (DL-PFC). This method was a key component of Nolan Williams’ groundbreaking SAINT-TRD protocol. However, challenges remain, particularly in the complexity of functional MRI procedures and their reproducibility. 9
The SAINT – TRD protocol has been developed by Stanford University, USA
The protocol, known as Stanford Accelerated Intelligent Neuromodulation Therapy for Treatment-Resistant Depression (SAINT-TRD) 37, administers a total of 50 TMS treatments over five days. Each patient receives 10 TMS sessions daily, spanning approximately 10 hours per day.
By the end of the treatment week, over 90% of participants achieved full remission—not just symptom improvement, but complete resolution of depression and suicidal ideation. 12
Unlike structural MRI, functional MRI requires patients to remain still for extended periods to assess motor and language functions, making it impractical for individuals with claustrophobia or difficulty lying still. In such cases, a non-MRI-based navigation system serves as a viable alternative.
Interpretation of functional connectivity MRI can be challenging. It requires specialized expertise from a neuroradiologist and may present challenges in consistently reproducing functional MRI readings.
More facts on Accelerated TMS Protocols
Accelerated TMS refers to a treatment approach where patients undergo multiple TMS sessions per day, with some protocols including up to ten sessions daily over a five-day period. By condensing the treatment schedule, accelerated TMS provides faster relief from depressive symptoms compared to standard TMS.
A 2010 study on an accelerated TMS protocol found it to have an excellent safety profile, with efficacy comparable to standard daily TMS.
There are a few potential accelerated TMS protocols.
One approach involves administering multiple daily sessions of intermittent theta burst stimulation (iTBS).
The most prominent Accelerated TMS protocol is Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT), an experimental approach for treatment-resistant depression. SAINT delivers a higher number of pulses to the brain within a shorter timeframe to alleviate depressive symptoms. In a study led by Dr. Nolan Williams involving 21 hospitalized patients, 19 out of 21 participants achieved remission by the end of the fifth day.
The second most common accelerated TMS protocol utilizes conventional TMS (or repetitive TMS, rTMS) but increases the frequency of sessions from once per day to multiple sessions within a single day.
Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) is an advanced form of transcranial magnetic stimulation (TMS) designed to treat individuals with treatment-resistant depression (TRD).This protocol enhances traditional TMS by delivering high-dose intermittent theta-burst stimulation (iTBS) in a condensed timeframe, utilizing functional MRI (fMRI) to precisely target the stimulation. 38
Key Features of the SAINT Protocol:
- Personalized Targeting: SAINT employs resting-state fMRI to identify the optimal region within the left dorsolateral prefrontal cortex (DLPFC) for each patient. This area is selected, based on its functional connectivity with the subgenual anterior cingulate cortex (sgACC), a region implicated in mood regulation. 51
- Accelerated Treatment Schedule: The protocol administers 10 daily sessions of iTBS, each lasting approximately 10 minutes, with 50-minute intervals between sessions, over five consecutive days. This accelerated approach contrasts with traditional TMS protocols that typically require daily sessions over several weeks.
- High-Dose Stimulation: Each session delivers 1,800 magnetic pulses at 90% of the resting motor threshold, resulting in a cumulative high-dose stimulation intended to enhance therapeutic efficacy.
Efficacy and Safety of SAINT Protocol:
The Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) protocol is an innovative transcranial magnetic stimulation (TMS) approach specifically developed for treating treatment-resistant depression. This accelerated, high-dose intermittent theta-burst stimulation (iTBS) approach utilizes functional connectivity MRI (fcMRI) to precisely target the left dorsolateral prefrontal cortex (DLPFC), enhancing treatment efficacy.
Efficacy: In an open-label study involving 22 participants with treatment-resistant depression, SAINT demonstrated a remission rate of approximately 86.4%, with 19 out of 22 participants meeting remission criteria. Notably, neuropsychological assessments indicated no adverse cognitive effects following treatment. 53
Safety: The SAINT protocol was well-tolerated among participants, with no significant adverse events reported. The treatment was associated with minimal side effects, primarily mild headaches and scalp discomfort, which are common with TMS procedures. Importantly, there were no reports of negative cognitive side effects or the emergence of manic symptoms during the study. 53
While these initial findings are promising, the authors emphasize the need for larger, double-blinded, sham-controlled trials to confirm the observed remission rates and further establish the safety profile of the SAINT protocol.
Navigated Transcranial Magnetic Stimulation: Advancing Mental Health Treatment
It’s a proven fact that TMS works where medication fails. It all depends on the accuracy of mapping of a patient brain which means to identify patient’s’ treatment targets better.
Consistency in stimulating these targets gives out consistent result and avoiding side effects associated with stimulating unwanted targets. The future of navigated TMS is very bright as lots of researches are working on this subject. 9
Difference Between Navigated TMS (nTMS) and Repetitive TMS (rTMS)
Navigated Transcranial Magnetic Stimulation (nTMS) and Repetitive Transcranial Magnetic Stimulation (rTMS) are both non-invasive brain stimulation techniques, but they serve different purposes in clinical and research settings.
Key Differences Between nTMS and rTMS
| Feature | nTMS (Navigated TMS) | rTMS (Repetitive TMS) |
| Primary Purpose | Used for brain mapping and diagnostics, mainly in neurosurgical planning and research. | Used for therapeutic neuromodulation, mainly in psychiatric and neurological treatments. |
| Mechanism | Delivers single or paired pulses to specific brain regions to assess function. | Delivers repetitive pulses to modulate brain activity over time. |
| Navigation System | Uses MRI-guided neuronavigation for precise targeting of cortical areas. | Does not require MRI guidance; uses standard anatomical landmarks for coil placement. |
| Applications | – Preoperative brain mapping (e.g., for brain tumours, epilepsy, stroke). – Motor and speech cortex mapping. – Research in neurophysiology. – Diagnosis of neuromuscular disorders. |
– Treatment of major depressive disorder (MDD), OCD (Obsessive compulsive disorder), and chronic pain. – Investigated for conditions like PTSD, anxiety, and schizophrenia. – Neuroplasticity enhancement for stroke recovery. |
| Depth of Stimulation | Similar to rTMS, stimulates superficial cortical structures (~0.7 cm). | Also targets superficial brain areas, but with repetitive pulses to induce long-term changes in neural activity. |
| Stimulation Type | Single-pulse or paired-pulse TMS for real-time functional assessment. | High-frequency (excitatory) or low-frequency (inhibitory) repetitive stimulation. |
| FDA Approval | Approved for preoperative motor and speech mapping. | FDA-approved for depression (2008), OCD (2018), migraine (2013). |
| Patient Experience | Short-duration sessions for assessment, not for treatment. | Typically requires daily sessions for several weeks for therapeutic benefits. |
Navigated brain stimulation (NBS)” and “navigated TMS” are effectively interchangeable terms (synonymous).
Development of navigated brain stimulation (NBS) is relatively a recent phenomenon to facilitate the use of TMS more accurately to the affected area of brains. FDA has approved these types of TMS already.
- Navigated Brain Stimulation (NBS) Development
- A relatively recent advancement to improve the accuracy of TMS application.
- FDA-approved for clinical use.
- Advantages of NBS Over Traditional TMS
- Traditional TMS activates a broad cortical area, making precise stimulation difficult.
- NBS, when combined with MRI-based navigation, allows targeted stimulation of specific anatomical areas of the cortex.
- Use of TMS for Cortical Assessment
- TMS is a non-invasive method for assessing cortical physiology and descending motor pathways.
- Motor evoked potentials (MEPs) are commonly used to measure peripheral muscle responses to TMS.25
- Components of NBS Devices
- Infrared camera detects trackers placed on a headband (worn by the subject) and on the TMS coil.
- MRI-based data enables the reconstruction of a 3D model of the subject’s head.
- Some devices can measure the strength and direction of the electric field induced in the brain by TMS.
- Expanding the Scope of TMS with NBS
- Enhances TMS measurement and allows reliable stimulation of additional brain regions.
- Enables stimulation of the premotor cortex, cerebellum, sensory areas, and cognitive areas.18
- Growing Role of TMS in Neuroscience and Medicine
- Recognized as a valuable tool for studying brain function.
- A promising treatment for neurological and psychiatric disorders.
- Expected to play a significant role in personalized mental health care.
- Offers hope for patients with treatment-resistant conditions as research progresses.
DEEP TMS
Deep transcranial magnetic stimulation, or deep TMS, that uses gentle magnetic waves to stimulate nerve cell activity in deeper and broader areas of the brain by using H coils. This brain stimulation can have pronounced effects on mood and behaviour, improving symptoms of major depression and other mental health disorders. Deep TMSTM utilizes specially designed H-Coils to induce neuronal depolarization in deep and wide cortical regions.14
Deep transcranial magnetic stimulation (dTMS) is relatively a new technology allowing non-surgical stimulation of relatively deep brain areas. Deep TMS is an effective treatment for a range of mental health and medical conditions, like
- Major Depressive Disorder
- Anxiety
- Obsessive-compulsive-disorder
In the European Economic Area (EEA), various types of deep TMS with H-coils are CE-marked for the treatment of bipolar disorder, chronic pain, epilepsy, Parkinson’s disease, Alzheimer’s disease, and post-traumatic stress disorder (PTSD)., schizophrenia, and smoking cessation. 14
FDA has cleared MDD and OCD for Deep TMS
WHAT IS THE DIFFERENCE BETWEEN rTMS and Deep TMS (dTMS)
Although a controversy still exists between the efficacy of rTMS and dTMS, off late it is increasingly found that dTMS is more effective although for the fact that both are FDA (rTMS in 2008 and dTMS in the year 2013) approved.
Repetitive transcranial magnetic stimulation (rTMS) and deep transcranial magnetic stimulation (dTMS) are both non-invasive brain stimulation techniques approved by the U.S. Food and Drug Administration (FDA) for treating mental health conditions. However, they differ in coil design, depth of stimulation, and clinical efficacy.
Regulatory Approval and Clinical Applications
- rTMS was FDA-approved in 2008 for major depressive disorder (MDD).
- dTMS received FDA approval in 2013 and has expanded indications, including obsessive-compulsive disorder (OCD).
- dTMS has also received the CE mark for use in the European Economic Area (EEA) for conditions beyond MDD and OCD, such as:
- Alzheimer’s disease (AD)
- Autism
- Bipolar disorder
- Chronic pain
- Multiple sclerosis (MS)
- Parkinson’s disease
- Post-stroke rehabilitation
- Post-traumatic stress disorder (PTSD)
- Negative symptoms of schizophrenia
- Smoking cessation
Key Technical Differences
|
Effectiveness and Safety
- rTMS delivers targeted stimulation but is limited in depth and spatial coverage, which can result in missing deeper brain structures related to psychiatric and neurological disorders.
- dTMS reaches deeper brain regions and stimulates a larger volume, making it more effective for conditions involving subcortical structures, as evidenced by a 2014 Brain Stimulation study.
- Both techniques are safe and well-tolerated, but dTMS offers a potential advantage in treating resistant cases due to its ability to engage a broader network of neural circuits. While both rTMS and dTMS are effective, dTMS has demonstrated superior efficacy in reaching deeper brain regions and treating a wider range of conditions. As research continues, dTMS may play a growing role in personalized treatment strategies for neurological and psychiatric disorders.15
Quadri-pulse Stimulation
Quadri pulse Stimulation (QPS) is an advanced form of repetitive transcranial magnetic stimulation (rTMS) designed to modulate cortical excitability and induce neural plasticity in humans (Kaneko et al., 2020).
Quadripulse transcranial magnetic stimulation (QPS) is an advanced form of repetitive transcranial magnetic stimulation (rTMS) designed to modulate cortical excitability (Kaneko et al., 2020). This technique involves administering four bursts of monophasic TMS using four independent magnetic stimulators, with each burst followed by a five-second inter-burst interval (IBI).
The inter-pulse intervals (ISIs) within each burst are crucial, as shorter ISIs (e.g., 5 milliseconds) tend to enhance cortical excitability, while longer ISIs (e.g., 50 milliseconds) are more likely to suppress it. 44
Compared to other non-invasive brain stimulation protocols, QPS demonstrates lower variability in its after-effects. Studies indicate that approximately 80% of younger participants respond to QPS-50ms, with 69% exhibiting measurable changes in motor evoked potentials (MEPs) (Hanajima et al., 2017; Nakamura et al., 2017). This reliability in modulating cortical excitability is attributed to the use of repetitive monophasic pulses rather than biphasic pulses, as seen in rTMS. 45
Monophasic pulses not only produce stronger effects on MEPs but also sustain these effects for over an hour. Their use in QPS likely contributes to the reduced variability observed compared to biphasic rTMS protocols, as well as the higher proportion of responders following QPS application. 16
QPS has been investigated for its therapeutic potential in various neurological and psychiatric disorders, including Parkinson’s disease, epilepsy, cerebrovascular disease, and major depression. Its ability to induce robust and reliable neural plasticity makes it a promising tool for both research and clinical applications. 46
In summary, Quadripulse Stimulation represents a significant advancement in non-invasive brain stimulation techniques, offering precise control over cortical excitability and opening new avenues for understanding and treating disorders associated with neural plasticity.
This method may solve some of the major obstacles in achieving treatment efficacy for “rTMS-resistant” patients. The new emerging method of QPS (Quadripulse Stimulation) that has shown higher efficacy in motor cortical plasticity than the previous methods.
Mechanism and Effectiveness of Coils
TMS & Neuronal Activities: TMS operates through a coil placed against the scalp, which generates magnetic pulses. These pulses induce small electrical currents in the brain, stimulating underactive neurons associated with mood disorders. For instance, low-frequency repetitive TMS (rTMS) has been shown to modulate neuronal activity and functional connectivity across different brain regions, as indicated by changes in c-Fos expression. 54
Over multiple sessions, this repeated stimulation helps to restore normal brain activity, leading to improved mental health outcomes.
The stimulation process involves targeting specific areas of the dorsolateral prefrontal cortex (DLPFC), which is often underactive in individuals suffering from depression. The induced electrical currents help modulate neurotransmitter levels, particularly dopamine, serotonin, and norepinephrine, which play crucial roles in mood regulation (Pascual-Leone et al., 2002).
Additionally, studies in The Journal of Clinical Psychiatry (Lisanby et al., 2008) suggest that TMS not only improves mood but also positively impacts cognitive function, making it a promising treatment for various psychiatric and neurological disorders. Other research highlights TMS’s potential in influencing synaptic plasticity, which is crucial for long-term mood stabilization and cognitive enhancement (Fitzgerald et al., 2006).
According to research published in Biological Psychiatry (George et al., 2010), the stimulation of the prefrontal cortex using TMS leads to increased neuronal activity, promoting neuroplasticity and enhancing communication between different brain regions. This process is particularly beneficial for individuals suffering from depression, where certain areas of the brain may exhibit reduced activity. Furthermore, studies in The Journal of Clinical Psychiatry (Lisanby et al., 2008) suggest that TMS not only improves mood but also positively impacts cognitive function, making it a promising treatment for various psychiatric and neurological disorders.
Despite its broad application, the exact neurophysiological mechanisms of TMS are not yet fully understood. Research combining TMS with neuroimaging techniques, such as functional magnetic resonance imaging (fMRI) and electroencephalography (EEG), aims to elucidate how TMS influences brain activity and connectivity. These multimodal approaches provide insights into the causal relationships between neural circuits and behaviour, enhancing our understanding of TMS’s impact on neural dynamics. 55
Structure of Coils in Transcranial Magnetic Stimulation (TMS) Treatment
Since Coils play a fundamental role in Transcranial Magnetic Stimulation (TMS) by generating the magnetic fields necessary to induce electrical activity in targeted brain regions, the effectiveness, depth of stimulation, and focality of TMS treatment largely depend on the design, shape, and positioning of the coil used.
Mechanism of Action
TMS coils create rapidly changing magnetic fields that penetrate the scalp and skull to induce an electric current in underlying cortical neurons. This induces or modulates neural activity without the need for direct electrical contact.
Types of Coils Used and When
TMS devices use different types of coils to generate magnetic fields, each designed for specific applications and depths of brain stimulation.
According to a study published in Brain Stimulation (Rossi et al., 2020), coil design significantly influences treatment outcomes, with deeper coils demonstrating enhanced efficacy for disorders involving subcortical structures.
- Circular coil Produces broader and less focal stimulation, mainly used in research to explore cortical excitability. Large-field repetitive transcranial magnetic stimulation with circular coil in the treatment of functional neurological symptoms (FNS) or Functional Neurological Disorder (FND):
- Chronic pain conditions, such as fibromyalgia, back and neck pain, and complex regional pain syndrome.
- Persistent fatigue.
- Sleep disturbances, including insomnia (insufficient sleep) and hypersomnia (excessive sleep).
- Migraines and other forms of headache and facial pain.
- Figure-eight coil: The most commonly used coil in repetitive TMS (rTMS), it provides focused and shallow stimulation, ideal for targeting the dorsolateral prefrontal cortex in depression treatment. 19
The Role of Figure-Eight Coils in TMS from Focal to Deep Stimulation, offers significant advantages in localized brain stimulation. This coil design has been instrumental in studies on functional brain organization, neuronal connectivity, and cortical plasticity 33, making it a widely adopted tool in both basic and clinical medicine.
Building on the success of TMS, repetitive TMS (rTMS)—which delivers repeated pulses—has been introduced as a potential treatment for chronic pain, depression, Parkinson’s disease, and neurorehabilitation. Treating these conditions often requires stimulation of deeper brain structures, leading to advancements in coil design that enhance both stimulation depth and focality. While figure-eight coils excel in targeted and directional stimulation, round coil configurations are primarily concerned with increasing depth and energy distribution.
Originally developed for non-invasive and focal brain stimulation, the figure-eight coil has significantly contributed to functional brain mapping and neuroscience research. Over time, its role has expanded into therapeutic applications, particularly through rTMS. Systematic studies on coil design continue to demonstrate the figure-eight coil’s ability to balance focal precision with sufficient depth of induced fields.
As TMS technology evolves, the figure-eight coil remains a cornerstone in both neuroscience and clinical medicine, with ongoing technological advancements expected to further refine its applications and effectiveness.19
- Double-Cone Coils: Advancing Deep Brain Stimulation
The double-cone coil, designed with large, angled windings, has been developed to modulate deeper brain regions, including the anterior cingulate cortex (ACC). As an enhanced version of the figure-eight coil, it provides greater penetration depth while sacrificing some focal precision. This allows it to target areas inaccessible to traditional figure-eight coils, such as the leg motor cortex, medial prefrontal cortex, cingulate gyrus, insula, and cerebellum.
In clinical studies, the use of double-cone coils has not been associated with serious adverse events. Several models have received FDA and CE certification, expanding their application in the treatment of conditions such as obsessive-compulsive disorder (OCD).
Design and Functionality
- The figure-eight coil consists of two adjacent circular coils in the same plane.
- The double-cone coil, by contrast, features two circular coils angled at 120°, enhancing its ability to reach deeper neural structures. 20
Clinical Applications of Double-Cone Coils
- Lower limb motor dysfunction
- Depression
- Obsessive-compulsive disorder (OCD)
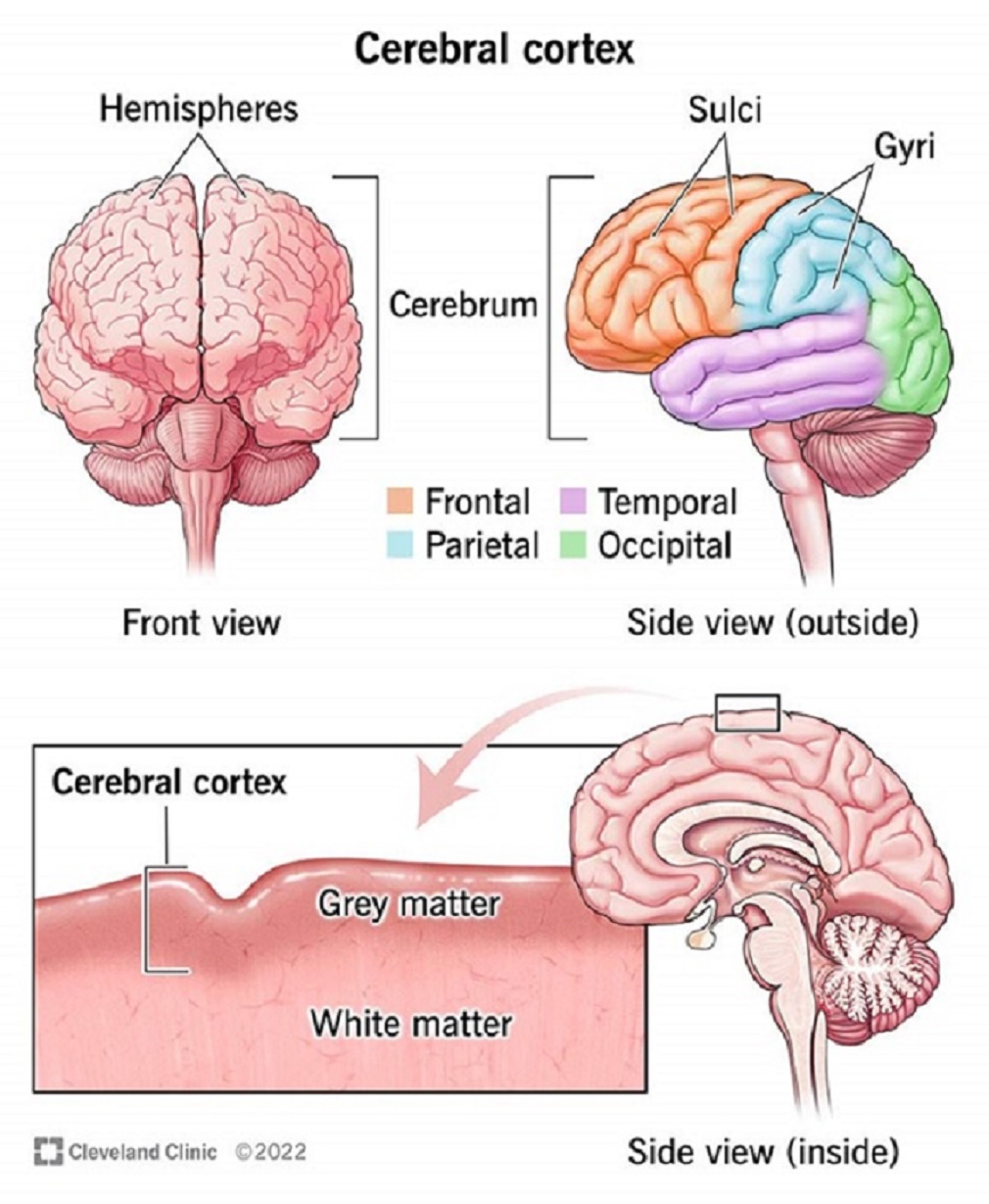
Understanding the Cerebral Cortex
- The cerebral cortex, also known as Gray matter, is the brain’s outermost layer of nerve tissue. Characterized by its gyri (folds) and sulci (grooves), it plays a crucial role in memory, cognition, learning, reasoning, problem-solving, emotions, and sensory processing.
- The human cerebral cortex consists of six layers and is divided into four major lobes, each responsible for processing different types of information:
- Frontal lobe – Executive functions, decision-making, motor control, and personality.
- Parietal lobe – Sensory processing, spatial awareness, and movement coordination.
- Temporal lobe – Auditory processing, language comprehension, and memory.
- Occipital lobe – Visual processing and interpretation.21
As research into double-cone coils progresses, their ability to stimulate deep brain structures may lead to expanded applications in neurology and psychiatry, further advancing non-invasive brain stimulation therapies.
[Circular coils are ideal for stimulating large and superficial motor areas, such as those associated with upper-limb movement. In contrast, the figure-of-eight coil delivers more focused stimulation, with the maximum electric field concentrated at its centre (hot spot), where the two loops intersect, enabling precise targeting of specific areas. Meanwhile, double-cone coils are designed to penetrate deep cortical layers, making them particularly suitable for stimulating the motor regions of the lower limbs, which are located deep within the interhemispheric fissure.] 18
- Air Cooled Coil – An air-cooled coil in a transcranial magnetic stimulation (TMS) system is designed to manage heat dissipation effectively during prolonged stimulation sessions. The coil, which generates rapidly changing magnetic fields, can overheat due to Joule heating. To prevent excessive heating, forced air cooling is often used as an efficient thermal management solution.
Key Aspects of Air-Cooled Coils in TMS Systems:
Coil Structure
- Typically made of copper or litz wire to optimize electrical efficiency.
- Encased in insulation material to prevent electrical leakage and improve durability.
Cooling Mechanism
- Forced-Air Cooling: Fans or blowers push air across the coil to dissipate heat.
- Heat Sinks: Some designs incorporate aluminum or copper heat sinks to aid cooling.
- Ventilation Design: The coil housing includes perforations or ducts for airflow.
Advantages of Air-Cooled Coils in TMS
- Cost-Effective: Cheaper than liquid-cooled alternatives.
- Lightweight: Easier to integrate into portable or wearable TMS systems.
- Reliability: Less complex than water-cooled systems, reducing the risk of leaks or mechanical failures.
Performance Considerations
- Power Handling: Higher-intensity TMS sessions require efficient cooling to maintain performance.
- Noise Levels: Fans may introduce operational noise, which is a factor in clinical and research settings.
- Temperature Regulation: Sensors may be integrated to monitor coil temperature and adjust airflow dynamically. 34
- C-Core coil and circular crown coil – Two coil configurations potentially suitable for dTMS are analysed: circular crown coil and C-core coil. These coils have significantly less attenuation of the electric field strength in depth, compared to conventional TMS coils. 35
A crown coil and a C-shaped coil are distinct types of transcranial magnetic stimulation (TMS) coils, each designed for different applications and stimulation characteristics.22
- C-Shaped Coil
- Named for its “C” shape, this coil design incorporates a ferromagnetic core, which helps concentrate and direct the magnetic field more effectively.
- Provides focused, deep brain stimulation while improving energy efficiency.
- Commonly used in deep TMS (dTMS) systems for treating conditions like depression and OCD.
- Crown Coil
- More circular in design, with a wider and flatter top resembling a crown.
- Designed to reach deeper brain regions, such as the subgenual anterior cingulate cortex (sgACC) and other subcortical areas.
- Often used in advanced TMS research for targeting hard-to-reach brain structures.
Key Differences
| Feature | C-Shaped Coil | Crown Coil |
| Shape | Resembles letter “C” | Round with a flat, wide surface |
| Magnetic Field | Concentrated and directed | Wider and deeper penetration |
| Stimulation Depth | Deep, but more focal | Even deeper brain stimulation |
| Application | Deep TMS (dTMS) for neuropsychiatric conditions | Research applications for subcortical brain areas |
A C-core coil is a specialized coil design used in transcranial magnetic stimulation (TMS) to deliver targeted magnetic fields with improved efficiency and focality. Unlike circular or figure-eight coils, the C-core design incorporates a ferromagnetic core in a C-shaped structure, which enhances the magnetic flux concentration and reduces energy losses.
Key Characteristics of C-Core Coils in TMS
- Enhanced Magnetic Field Efficiency
- The ferromagnetic C-shaped core directs and amplifies the magnetic field, increasing efficiency compared to air-core coils.
- Higher magnetic flux density enables stronger and deeper stimulation with lower power input.
- Improved Focality
- Compared to conventional circular coils, C-core coils can focus the magnetic field more precisely, minimizing unwanted stimulation of surrounding areas.
- Useful for targeting deeper brain regions without excessive surface stimulation.
- Reduced Energy Consumption and Heat Generation
- The ferromagnetic core reduces energy dissipation, making the coil more energy-efficient.
- This leads to lower heat generation, reducing the need for extensive cooling systems.
- Applications in TMS Research and Clinical Use
- C-core coils are often used in deep TMS (dTMS) systems, such as those developed for treating major depressive disorder (MDD), obsessive-compulsive disorder (OCD), and other neuropsychiatric conditions.
- Certain designs enable bilateral stimulation or specific targeting of subcortical structures, which is crucial for certain therapeutic applications.
Comparison with Other Coil Types
| Coil Type | Stimulation Depth | Focality | Energy Efficiency | Cooling Requirements |
| Circular Coil | Shallow | Low | Moderate | High |
| Figure-8 Coil | Moderate | High | Moderate | Moderate |
| C-Core Coil | Deep | High | High | Low |
C-shaped miniaturized coil for transcranial magnetic stimulation for the small animals. Animal models play a crucial role in exploring the fundamental mechanisms of TMS.
Since most commercial coils are designed for humans and thus incapable of focal stimulation in small animals, it is difficult to perform electrophysiological recordings at the TMS focal point using conventional coils. C core coil is a solution for the animal segments. 36
5. Hesed-coil: Recently developed, used in deep TMS (dTMS), this coil allows deeper penetration into brain structures, within the temporal lobe. its innovative design features an array of elements precisely contoured to match the skull’s shape. This structure allows for the induction of deeper and more extensive stimulation volumes compared to traditional coil designs, enhancing the reach and effectiveness of transcranial magnetic stimulation (TMS), making it effective for treatment-resistant depression and conditions like obsessive-compulsive disorder (OCD). 23
Traditional TMS coils, such as the figure-eight design, primarily affect superficial cortical areas due to the rapid decline of the induced electric field with depth. In contrast, the H-coil’s unique configuration allows for a slower attenuation of the electric field, enabling it to reach deeper neural structures without necessitating excessively high stimulation intensities. 17
More precisely, Standard TMS coils, commonly used in research and clinical settings, are limited in their ability to directly stimulate deep brain structures. The magnetic fields generated by these coils diminish rapidly with depth, requiring extremely high intensities to reach deeper regions. However, such intensities would also cause excessive stimulation in cortical areas, leading to unwanted side effects. The H-coil overcomes this limitation by enabling deep brain stimulation (DBS) without excessively increasing intensity, thereby minimizing cortical overstimulation. 24
The H-coil was developed based on numerical simulations and phantom brain measurements to optimize its ability to target deeper brain regions. Studies have demonstrated that the H-coil can activate the motor cortex at depths of up to 5.5 cm, compared to approximately 2 cm with standard figure-eight coils. This capability makes the H-coil particularly suitable for deep TMS (dTMS) applications, expanding the range of treatable conditions. 36
Deep TMS (dTMS), utilizing H-coils, can penetrate up to 6 cm into the brain, reaching deeper layers of the motor cortex—including areas responsible for leg movement. However, accurately modeling the path of induced currents remains challenging due to variations in brain shape, density, and water content, which create a nonuniform magnetic field and conductivity throughout brain tissues.25
As research progresses, H-coil technology holds promise for advancing non-invasive deep brain stimulation, potentially transforming treatments for various neurological and psychiatric conditions.
According to a study published in Brain Stimulation (Rossi et al., 2020), coil design significantly influences treatment outcomes, with deeper coils demonstrating enhanced efficacy for disorders involving subcortical structures.
The development and application of the H-coil have been significant in advancing TMS technology, offering new avenues for non-invasive neuromodulation in both research and clinical settings.
Final Thoughts on Transcranial Magnetic Stimulation (TMS)
Transcranial Magnetic Stimulation (TMS) has emerged as a powerful, non-invasive tool for treating various neurological and psychiatric conditions, particularly depression. By harnessing targeted magnetic pulses, TMS offers an alternative for individuals who have not responded to traditional treatments, with growing research supporting its effectiveness and safety.
As advancements in neuroscience continue, TMS is evolving beyond depression treatment, with promising applications in anxiety, PTSD, chronic pain, and even cognitive enhancement. While it may not be a one-size-fits-all solution, its potential to reshape brain health and mental well-being is undeniable.
With continuous research and growing accessibility, TMS offers promising potential as an innovative, science-based therapy. As we move forward, could TMS revolutionize our approach to brain health? The future holds the answer, but the prospects are undoubtedly exciting.
References:
[1] Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS),by Wanalee Klomjai , Rose Katz , Alexandra Lackmy-Vallée , Annals of Physical and Rehabilitation Medicine, Volume 58, Issue 4, September 2015, Pages 208-213, [ScienceDirect]
[2] Brain Stimulation Therapies, National Institute of Mental Health, National Institute of Mental Health;
[3] Magnetic Resonance Imaging, Wikipedia;
[4] TMS, National Institute of Mental Health
[5] Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS),by Wanalee Klomjai , Rose Katz , Alexandra Lackmy-Vallée , Annals of physical and rehabilitation medicine, Volume 58, Issue 4, September 2015, Pages 208-213, [ScienceDirect]
[6] Transcranial Magnetic Stimulation (TMS): Potential Progress for Language Improvement in Aphasia, by Elizabeth E Galletta, PhD, Paul R Rao, PhD, and Anna M Barrett, MD, Top Stroke Rehabil. 2011 Mar-Apr; 18(2): 87–91. doi: 10.1310/tsr1802-87
[7] Theta-burst stimulation: a new form of TMS treatment for depression, Sung Wook Chung 1, Kate E Hoy, Paul B Fitzgerald, Depress Anxiety. 2015 Mar;32(3):182-92.
doi: 10.1002/da.22335. Epub 2014 Nov 28.[PubMed]
[8] Theta burst stimulation for the acute treatment of major depressive disorder: A systematic review and meta-analysis, Jeffrey D. Voigt, Andrew F. Leuchter & Linda L. Carpenter , Published: 28 May 2021, [Spring Nature]
[9] Florida TMS clinic,
[10] Navigated TMS in the ICU: Introducing Motor Mapping to the Critical Care Setting; Severin Schramm, Alexander F Haddad, Lawrence Chyall, Sandro M Krieg, Nico Sollmann, Phiroz E Tarapore; Brain Sciences, PubMed Central
Severin Schramm, Alexander F. Haddad, Lawrence Chyall, Sandro M. Krieg, Nico Sollmann, and Phiroz E. Tarapore , Published online 2020 Dec 18. doi: 10.3390/brainsci10121005, PMID: 33352857 [PubMed]
[11] An efficient and accurate new method for locating the F3 position for prefrontal TMS applications, William Beam, B.S., Jeffrey J. Borckardt, Ph.D., Scott T. Reeves, M.D., and Mark S. George, M.D., Brain Stimul. Author manuscript; available in PMC 2010 Jun 9, [PubMed]
[12] Remission of Depression in 1 Week Using Accelerated TMS, Rejuvenate TMS [RejuvinateTMS]
[13] Accelerated TMS, what is it, [MidCity TMS]
[14] Gia Miami
[15] BrainsWay
[16] BRAINBOX
[17] Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS),by Wanalee Klomjai , Rose Katz , Alexandra Lackmy-Vallée , Annals of physical and rehabilitation medicine, Volume 58, Issue 4, September 2015, Pages 208-213, [ScienceDirect]
[18] Comparison of Coil Designs for Transcranial Magnetic Stimulation of a Pig Model, Oluwaponmile F Afuwape, Jenna Runge, Sarah A Bentil, David C Jiles; PubMed
Zhi-De Deng , Angel V Peterchev, Sarah H Lisanby, Annu Int Conf IEEE Eng Med Biol Soc
. 2008:2008:5675-9. doi: 10.1109/IEMBS.2008.4650502.
[19] Figure-Eight Coils for Magnetic Stimulation: From Focal Stimulation to Deep Stimulation, References : Shoogo Ueno and Masaki Sekino
Frontiers in human neuroscience, Published online 2021 Dec 16. doi: 10.3389/fnhum.2021.805971
[20] YINGCHI, Things you need to know about double cone coil——one kind of TMS coils
Release time :2022-09-16,Source:support@yingchitech.com
[21] Cerebral Cortex, Cleveland clinic
[22] A C-shaped miniaturized coil for transcranial magnetic stimulation in rodents, Wenxuan Jiang, Robert Isenhart, Charles Y Liu, and Dong Song, Published online 2023 Mar 24. doi: 10.1088/1741-2552/acc097. [PubMed]
[23] H-coil repetitive transcranial magnetic stimulation for treatment of temporal lobe epilepsy: A case report. R. Gersner, L. Oberman, M.J. Sanchez, N. Chiriboga, H.L. Kaye, A. Pascual-Leone, M. Libenson , Y. Roth , A. Zangen , A. Rotenberg Epilepsy & Behavior Case Reports
Volume 5, 2016, Pages 52-56. [ScienceDirect]
[24] Transcranial magnetic stimulation of deep brain regions: evidence for efficacy of the H-coil, Abraham Zangen , Yiftach Roth, Bernhard Voller, Mark Hallett. Comparative Study
Clin Neurophysiol . 2005 Apr;116(4):775-9. doi: 10.1016/j.clinph.2004.11.008. Epub 2004 Dec 16.
[25] Three-dimensional distribution of the electric field induced in the brain by transcranial magnetic stimulation using figure-8 and deep H-coils, Yiftach Roth , Alon Amir, Yechiel Levkovitz, Abraham Zangen, J Clin Neurophysiol . 2007 Feb;24(1):31-8. doi: 10.1097/WNP.0b013e31802fa393.[PubMed]
[26] Theta Burst Stimulation (TBS) explained. Monarch Mental Health Group
[27] Recognizing the risks of brain stimulation. MAURITS VAN DEN NOORT , SABINA LIM, AND PEGGY BOSCH. 12 Dec 2014,Vol 346, Issue 6215,p. 1307,DOI: 10.1126/science.346.6215.1307-a
[28] Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin Neurophysiol. 2021 Jan; 132(1): 269–306. Published online 2020 Oct 24. doi: 10.1016/j.clinph.2020.10.003. [PubMed]
[29] Theta burst stimulation for the acute treatment of major depressive disorder: A systematic review and meta-analysis, Jeffrey D. Voigt, Andrew F. Leuchter & Linda L. Carpenter . Translational Psychiatry volume 11, Article number: 330 (2021), Published: 28 May 2021
[30] Single-pulse transcranial magnetic stimulation (sTMS) for the acute treatment of migraine: evaluation of outcome data for the UK post market pilot program; by Ria Bhola , Evelyn Kinsella, Nicola Giffin, Sue Lipscombe, Fayyaz Ahmed, Mark Weatherall & Peter J Goadsby
[31] Paired-pulse transcranial magnetic stimulation protocol applied to visual cortex of anaesthetized cat: effects on visually evoked single-unit activity; Vera Moliadze , Dimitrios Giannikopoulos , Ulf T Eysel , Klaus Funke; Pub Central
[32] The Role of the Dorsolateral Prefrontal Cortex for Speech and Language Processing
Ingo Hertrich, Susanne Dietrich, Corinna Blum, Hermann Ackermann
[33] Neuroplasticity, Matt Puderbaugh; Prabhu D. Emmady.; National Library of Medicine
[34] Accessory to dissipate heat from transcranial magnetic stimulation coils, PubMed Michel Belyk , Braxton K Murphy , Deryk S Beal
[35] A C-shaped miniaturized coil for transcranial magnetic stimulation in rodents; PubMed Central; Wenxuan Jiang, Robert Isenhart, Charles Y Liu, Dong Song
[36] Transcranial magnetic stimulation set-up for small animals, frontiers in Neuroscience, PubMed Central; Jaakko O Nieminen, Alexey S Pospelov, Lari M Koponen, Pauliina Yrjölä, Anastasia Shulga, Stanislav Khirug, Claudio Rivera;
[36] Transcranial magnetic stimulation of deep brain regions: evidence for efficacy of the H-coil, PubMed Abraham Zangen 1, Yiftach Roth, Bernhard Voller, Mark Hallett,
[40] A Systematic Review of the Safety and Tolerability of Theta Burst Stimulation in Children and Adolescents, PubMed Central, Rana Elmaghraby, Qi Sun, Can Ozger, Julia Shekunov, Magdalena Romanowicz, Paul E Croarkin
[42] Navigated transcranial magnetic stimulation for mapping the motor cortex in patients with rolandic brain tumours, PubMed; Satoshi Takahashi, Peter Vajkoczy, Thomas Picht;
[43] Navigated TMS in the ICU: Introducing Motor Mapping to the Critical Care Setting, PubMed Central; Severin Schramm, Alexander F Haddad, Lawrence Chyall, Sandro M Krieg, Nico Sollmann, Phiroz E Tarapore
[44] Quadripulse stimulation (QPS), PubMed; Hideyuki Matsumoto , Yoshikazu Ugawa
[45] Quadripulse Stimulation, BRAINBOX;
[46] Quadripulse stimulation (QPS), PubMed; Hideyuki Matsumoto , Yoshikazu Ugawa
[47] What is motor cortex, Wikipedia
[48] Cortical Excitability, ScienceDirect
[49] Neuroplasticity, Wikipedia
[50] What is synaptic plasticity, Queensland Brain Institute
[51] A role for primate subgenual cingulate cortex in sustaining autonomic arousal, Peter H. Rudebeck peter.rudebeck@mssm.edu, Philip T. Putnam, Teresa E. Daniels, +3, and Elisabeth A. Murray
[52] Theta Burst TMS Technology: Great Promise and a Lot to Learn, William M. McDonald, M.D. wmcdona@emory.edu Authors Info & Affiliations; The American journal of Psychiatry;
[54] Low intensity repetitive transcranial magnetic stimulation modulates brain-wide functional connectivity to promote anti-correlated c-Fos expression, Scientific Reports, Nature; Jessica Moretti, Dylan J. Terstege, Eugenia Z. Poh, Jonathan R. Epp, Jennifer Rodger

Debasis Chaudhuri